Diving history enthusiasts know that the problem of saving submarine crews, no longer able to resurface due to mechanical failures or damage following military operations, has for years represented a technological challenge that has engaged scientists and engineers and has led to the design of numerous underwater breathing apparatus. Often these devices were also used in commercial and sporting applications.
The most evident developments of this trend occurred precisely in our country (Italy) after the end of the Second World War where the first autonomous underwater breathing apparatus used in civil and sports applications were the AROs (oxygen self-contained breathing apparatus) recovered from surplus military material stocks.
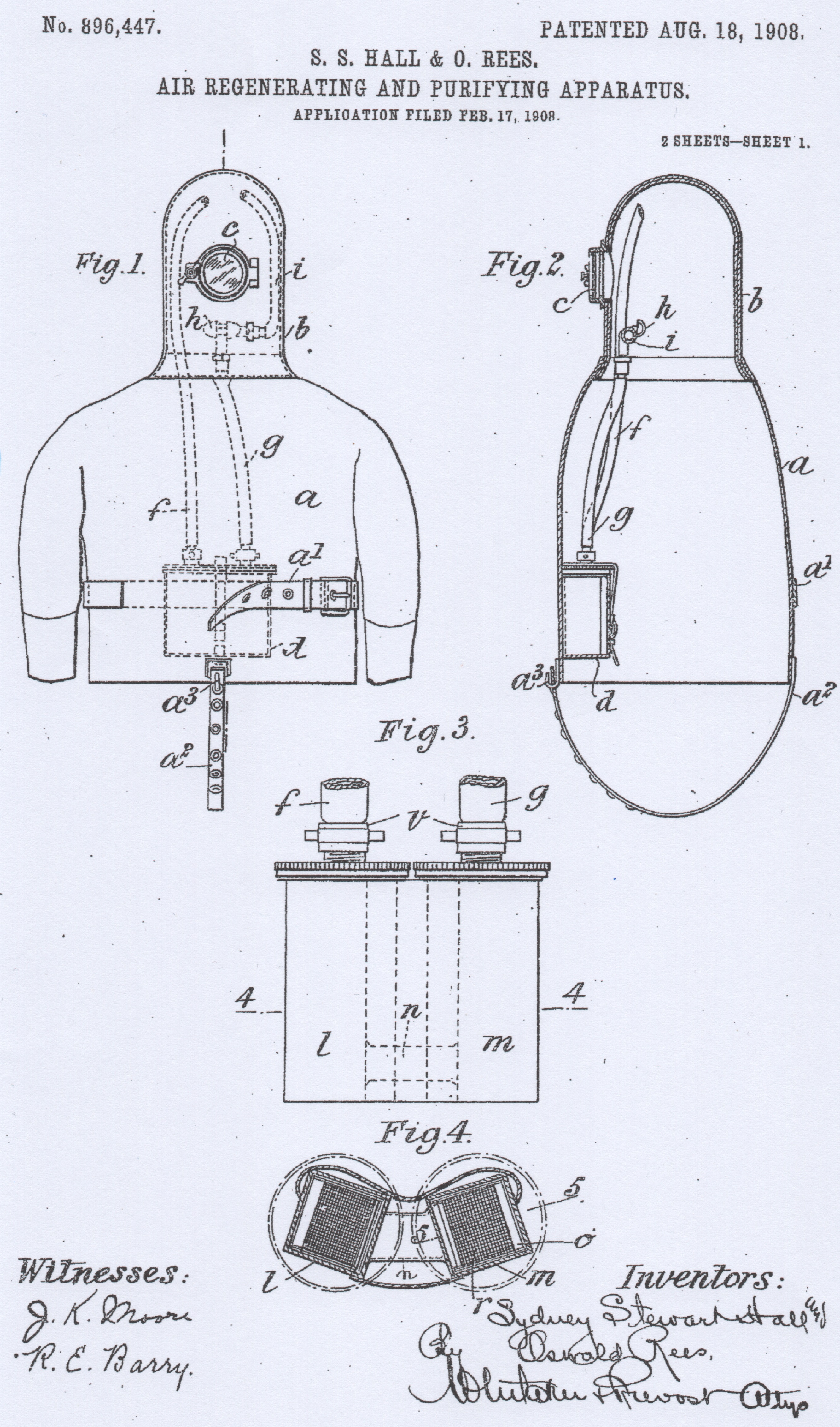
The very first solutions in this sector were developed in the United Kingdom as early as the first decade of the 1900s. In that period in England there were various proposals for emergency self-contained breathing apparatus to be used in toxic atmospheres (e.g. in the event of fire or inside mines) or for underwater applications. Among these, the one taken into consideration by the Royal Navy and the subject of specific tests for the rescue of submarine crews, was the Hall-Rees apparatus (fig. 1) patented in 1908 by captain Sidney Stewart Hall and the doctor Oswald Rees, both of the Royal Navy. The fig. 2 shows photos and drawings relating to some tests carried out with this device on the submarine HM C7 in 1909.
 |
 |
| fig. 1 | fig. 2 |
The device was then produced by Siebe & Gorman LTD, a famous British company led for several decades by Sir Robert H. Davis, Managing Director and owner of the company itself, but above all its main creative mind. And in fact this open diving apparatus was better known in subsequent years as the Hall-Rees-Davis device.
Davis continued to develop and further improve this device which, in 1927, was definitively adopted by the Royal Navy and subsequently also by other navies around the world (including the Italian Navy). Davis named it DSEA (Davis Submerged Escape Apparatus), and also patented it in the USA in the early 1930s. We talked about DSEA in details in a previous article.
The other European country that actively worked, since the beginning of the 1900s, on the development of a device with the same purposes was Germany. In particular, the national reference company for the design, development and production of this material was Dräger founded in Lübeck in 1889 by Johann Heinrich Dräger and Carl Adolf Gerling. And it was precisely in 1910 that the German Navy adopted the DM Tauchretter model oxygen rebreather.
After this overview of the European production of that period, let's now talk about the solution developed and adopted in the same period in the USA by the US Navy, the Momsen Lung.
The main reason that pushed me to write this article was the recent acquisition of even two units of this device, belonging to two different versions.
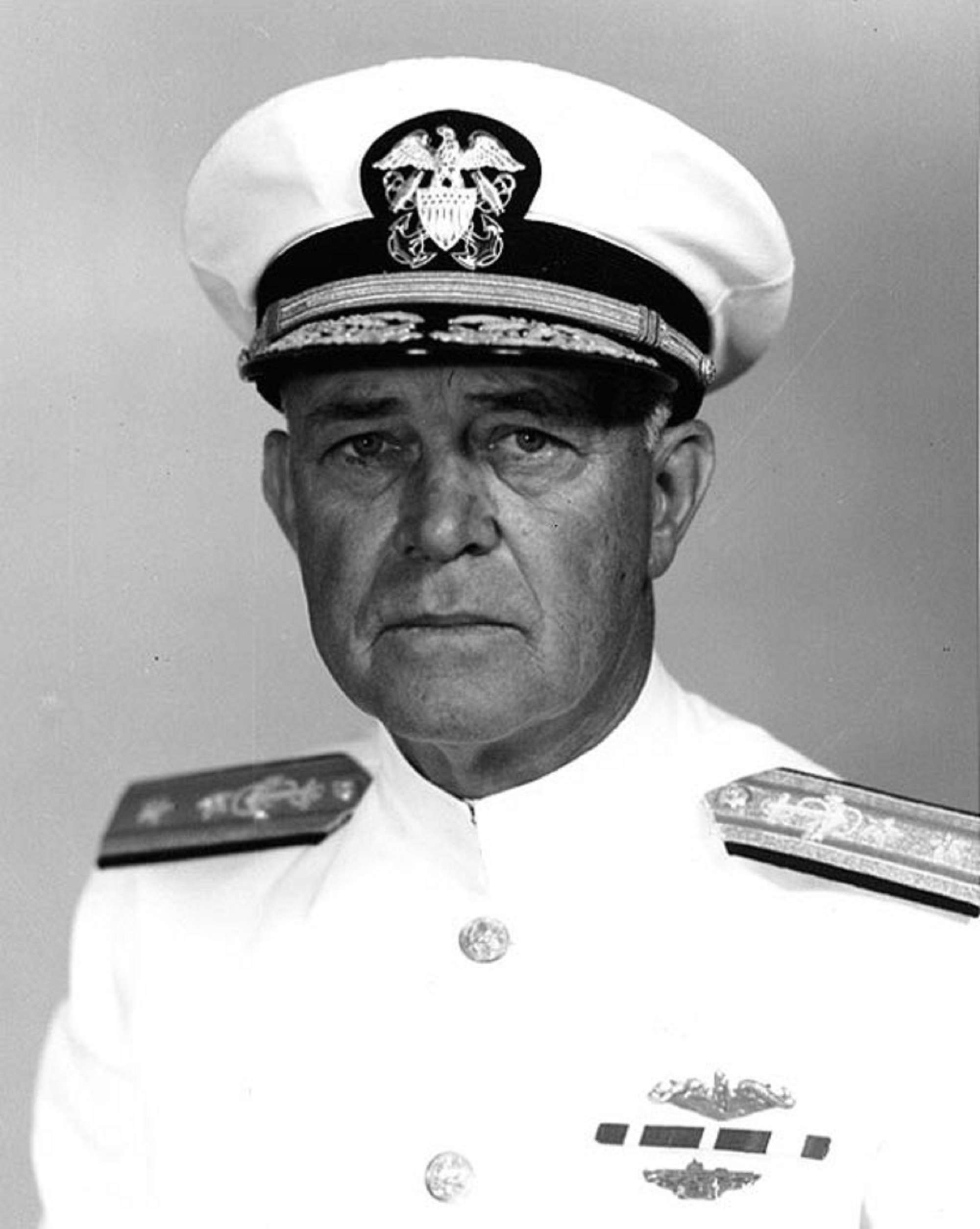
The Momsen Lung was invented by Charles Bowers Momsen (1896-1967), affectionately nicknamed “Swede” for his characteristic facial features (fig. 3). Momsen spent his entire career within the US Navy from 1916 to 1955, when he retired with the rank of Vice Admiral. The great vocation and dedication that Momsen put for much of his career in solving the problem of rescuing sailors trapped inside submarines stuck at the bottom had its sad baptism on 25 September 1925, when the submarine S-1 sank on a 40 meter bottom depth after being rammed by the City of Rome cargo ship. Two years later, in December 1927, another submarine, the S-4 (SS-109), sank off Cape Cod. Again, all 40 crew members could not be saved. Momsen began to study the problem from various points of view and followed two different design ideas.
The first was to develop a special diving bell (this equipment had already been in use since the previous century) capable of being lowered onto the submarine, positioned and made to adhere with a watertight seal at the exit hatch. After connection, the pressure inside the bell could be equalized with that inside the submarine, the hatch opened and finally the crew transferred and recovered.
The second idea instead concerned a self-contained breathing apparatus that the crew could wear before escaping the submarine and with which they could reach the surface safely. From this idea Momsen Lung would later be born.
The genesis and development phase of the special bell proved to be quite long, until it was finally completed in 1930 and officially adopted by the US Navy under the name of McCann Submarine Rescue Chamber (fig. 4).
 |
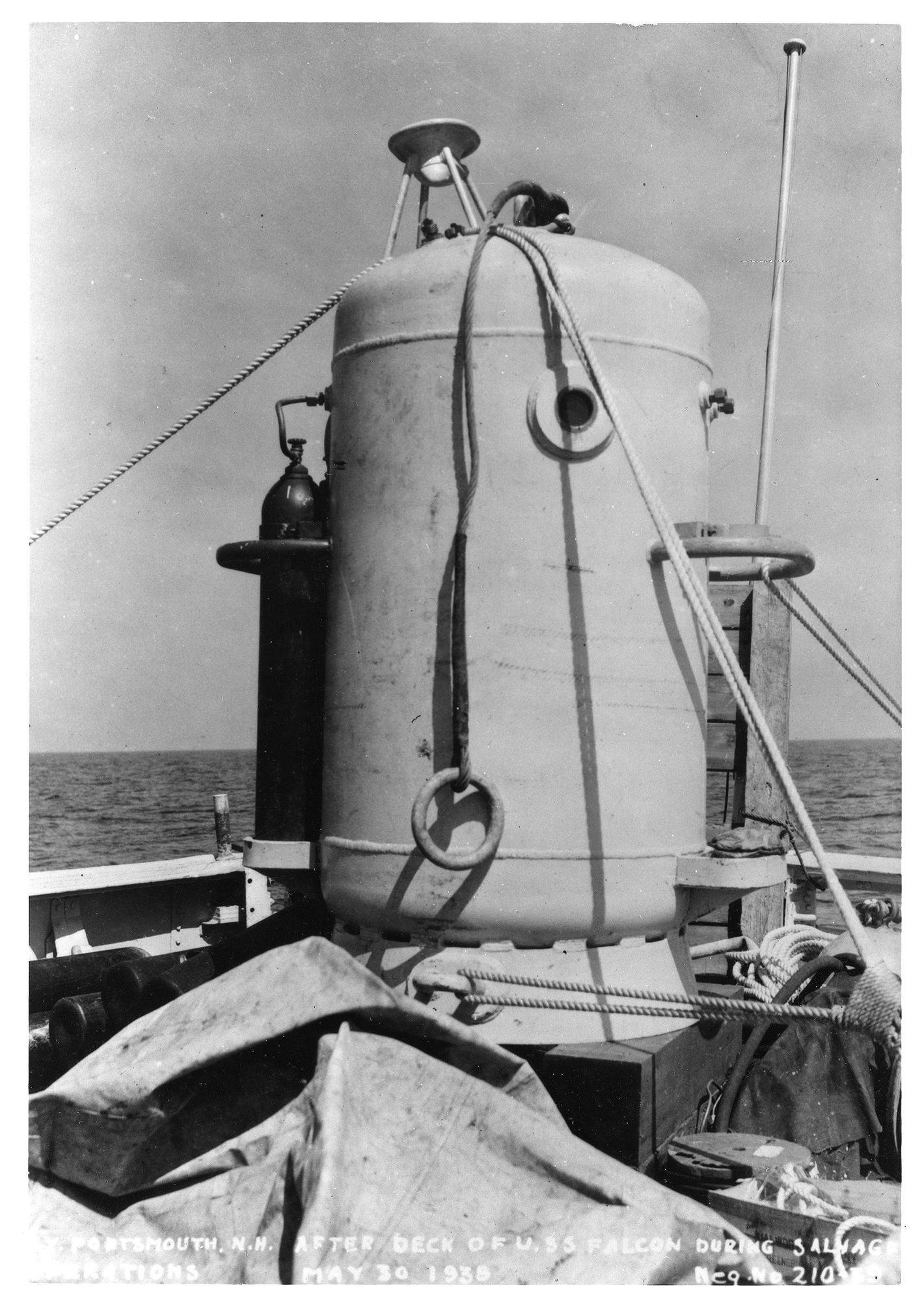 |
| fig. 3 | fig. 4 |
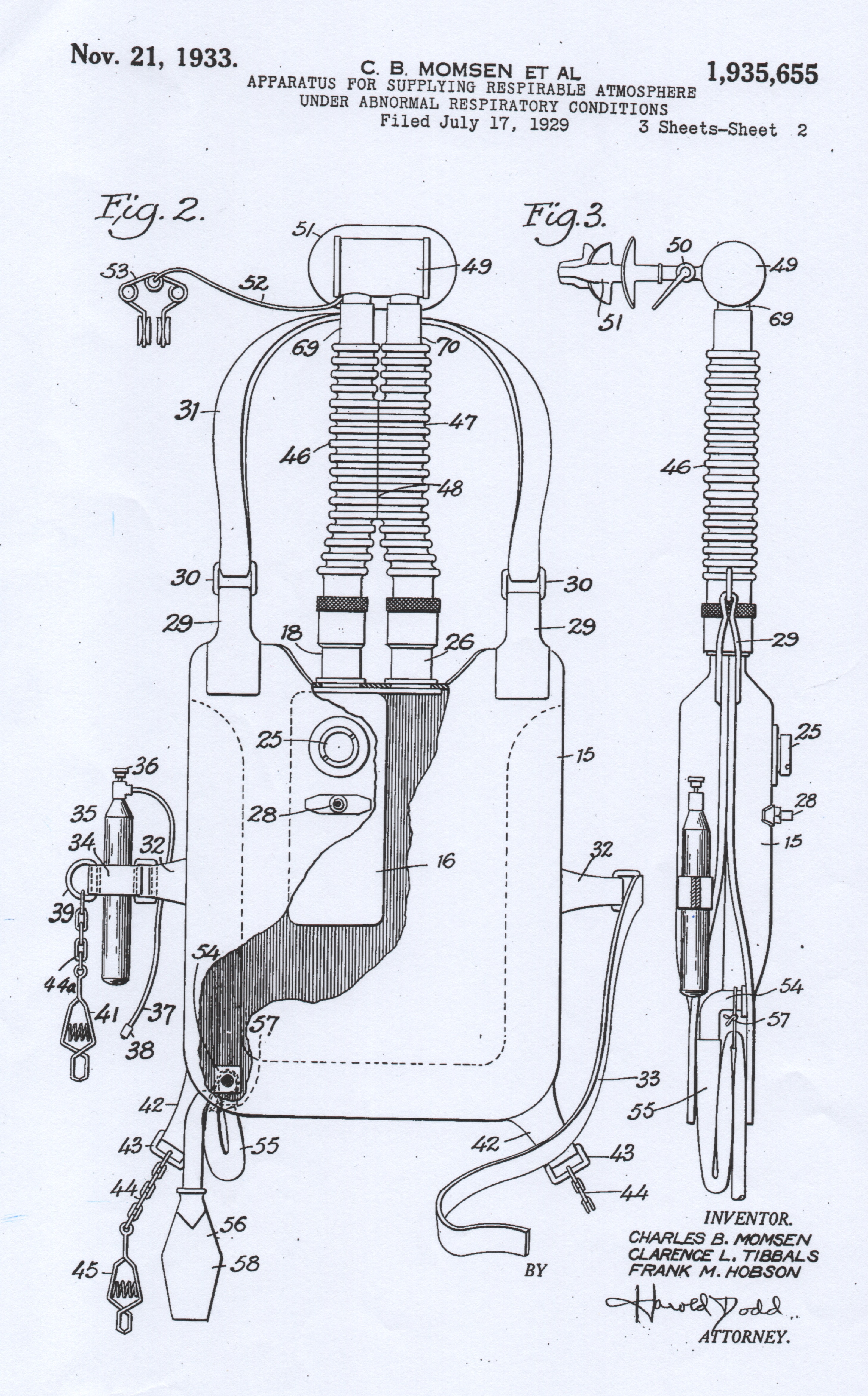
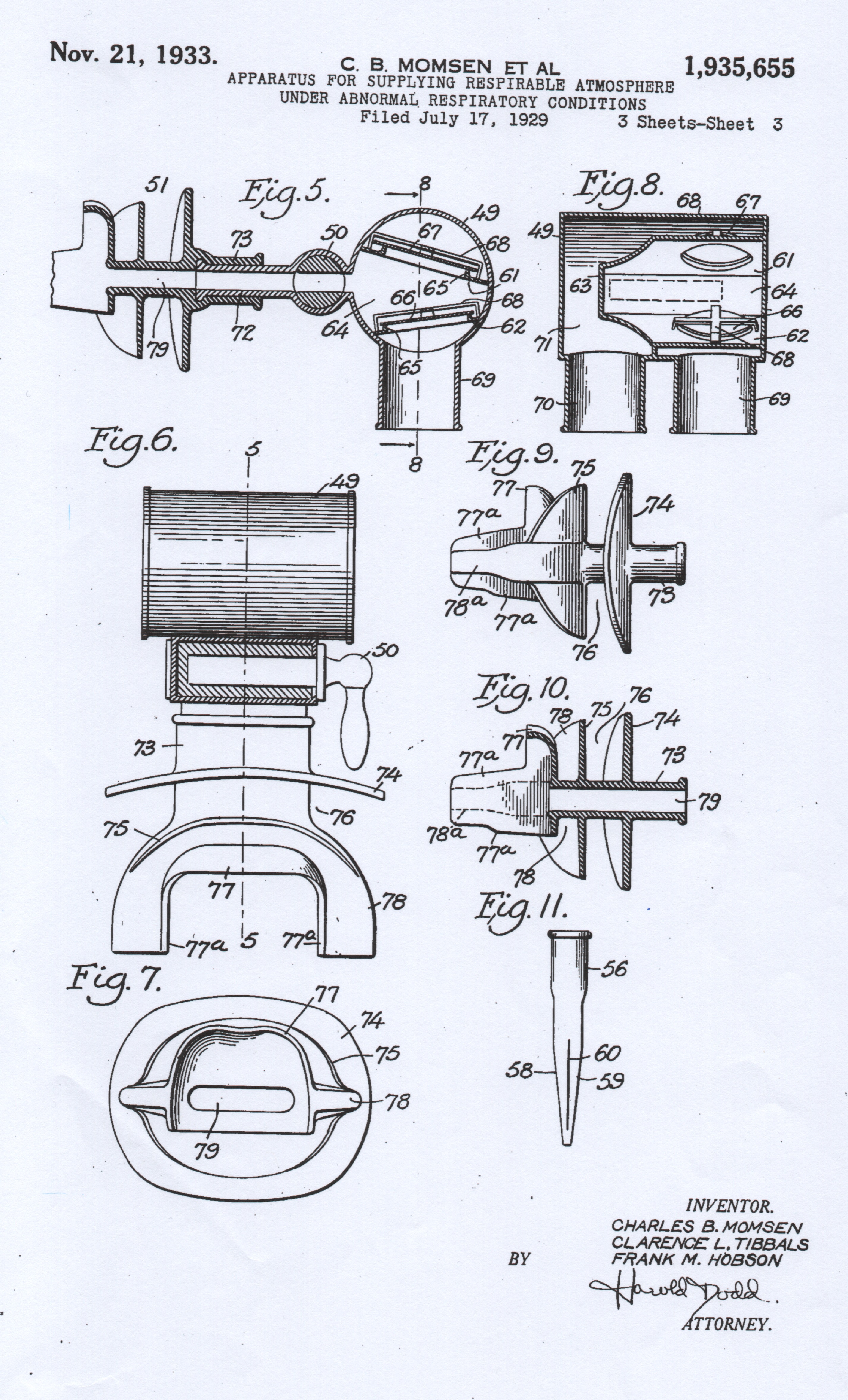
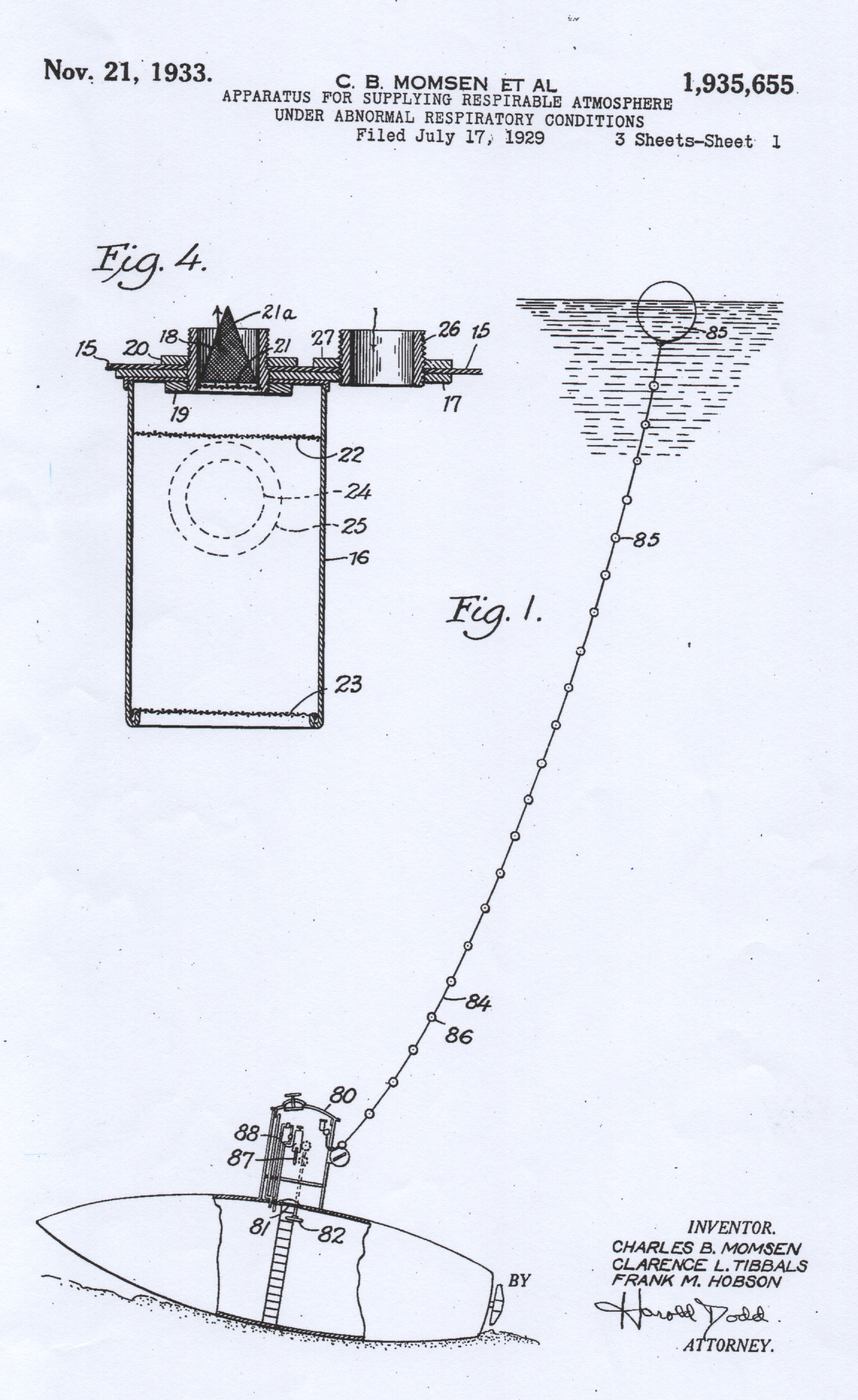
This special diving bell would later become famous during the recovery of the survivors of the submarine Squalus, which sank in May 1939 off the coast of New Hampshire at a depth of 74 meters. The entire rescue operation, which lasted 113 days and was headed by Momsen himself, allowed 33 crew members to be saved out of a total of 59 men. For those who want to dig deeper into this story, considered by many to be one of the greatest rescue operations in history, I recommend reading Peter Maas' book “The Terrible Hours: The Greatest Submarine Rescue in History – March 1, 2001”. To develop the second idea, Momsen enlisted the help of his friend Petty Officer Clarence L. Tibbals and Frank M. Hobson, a civilian employed in the Bureau of Construction and Repair (which later became the Bureau of Ships), the organization of the US Navy which took care of all the naval constructions intended for it. The research, design and validation test work lasted from June 1929 to September 1932 and also included an experimental dive with ascent from a depth of 200 feet (61 meters) for which Momsen received the Navy Distinguished Service Medal from the navy. In the same period, he and his collaborators submitted a patent application for this device, an application which was accepted on November 21, 1933 (fig. 5 and fig. 6). From the construction point of view and typical design solutions, this device is characterized by the following elements:
 |
 |
| fig. 5 | fig. 6 |
- It is a closed-circuit breathing apparatus that can work using both oxygen and air or even any mixture of nitrogen and oxygen.
- The device works by maintaining the breathing lung at a constant volume. This function is ensured by a duckbill exhaust valve located in the lower right part of the lung. During the ascent phase, the expanding volume of gas is discharged through said valve. In the prototype versions, and also in the patent description, this exhaust valve is installed at the end of a tube long enough to ensure that the air bag is maintained at a pressure slightly higher than ambient pressure. This solution was then abandoned for complexity reduction and ease of use.
- The gas used in the device is not supplied from a tank, as in the vast majority of similar devices, but is introduced into the breathing lung from an external source which is normally the compressed air circuit of submarines, or from separate tanks used for storage of oxygen or other gases. This quantity of gas remains the only resource used by the operator from the moment of activation and exit from the submarine to the end of the ascent phase.
- The respiratory circuit is cyclical with a canister containing soda lime placed inside the breathing lung on its right side and upstream of the inspiration line. The exhaled gas flows directly from the mouthpiece to the lung and is placed on its left side.
- The metal mouthpiece also includes one-way valves that regulate the direction of gas flow. The end part of the rubber mouthpiece is not equipped with a safety strap, as in the case of the DSEA, and is shaped in such a way as to prevent accidental loss of contact with the operator's mouth.
- A small valve is installed in the front part of the breathing lung, very similar to the one used to inflate car tires, which serves for the initial gas loading of the device.
- In a similar manner to that used in various similar models of breathing units, the device is secured to the operator's body by means of two distinct straps: one around the neck and another placed in the ventral area. The rather curious thing in this case is that two connection points with the lower edges of the lung have been added, formed by chains and clamps. These clamps can be quickly secured to the operator's suit and serve to prevent the bag from lifting in its lower part when immersed, creating difficulties of movement and higher breathing efforts.
- The tiny tank shown in fig. 5 is not part of the standard equipment of the device but is simply mentioned as a generic means for inflating the lung before exiting the submarine.
The thing that struck me most when reading the contents of the patent application and which is certainly atypical compared to other devices is the fact that this system does not involve the use of tanks or other gas storage devices to be used during the ascent phase. . The first question I asked myself was the following: could the initial gas contained in the lung bag be sufficient to ensure breathing and maintain the vital functions of the wearers in the main situations of use and for the expected operational depths? We have previously mentioned an experimental dive from a depth of 200 feet (61 meters), successfully carried out by Momsen's team. These doubts were amplified when, again in the patent application, I found the statement that this device, designed to maintain a constant volume of the lung bag regardless of depth, would be able to ensure respiratory function for any duration! But don't we consider the metabolic consumption of oxygen? The rather curious thing is that, to confirm and support the previous thesis, the example is given of an ascent starting from a depth of 300 feet (91 meters) with decompression stops every 10 feet (3 meters) starting from a depth of 70 feet (21 meters). Since the operator did not have a depth gauge and a timer at his disposal, the durations of these stops were defined with a specific number of breathing cycles, a number that varied depending on the depth of the stop. This procedure had to be carried out by remaining permanently in contact with a special line with small floating corks placed at intervals of 10 feet (3 meters), which the operator used to control the ascent speed and to understand the depth at which he was (and the consequent number of necessary breaths expected from that specific stop). As can be seen from the drawing contained in the patent documentation, this rope, kept tensioned by a float launched from the submarine before the evacuation, was secured at the crew exit hatch (fig. 7).
Driven by doubts relating to the effect of the metabolic consumption of oxygen in a volume of unreplenished gas, I started doing some calculations to understand if the ascent procedure set out in the patent pages was plausible. And my calculations have shown that already at the end of the stop at 60 feet (18 meters), the gas inside the lung bag is clearly hypoxic, therefore no longer capable of supporting the operator's vital functions. It is then evident that Momsen and his collaborators, in the initial phase of conception and development of the device, had rather vague ideas on the main laws of physiology and on the various implications in breathing oxygen in a hyperbaric environment. We then have to ask ourselves how the crew members, certainly under great psychophysical stress due to the extreme conditions and the drama of the situation, were able to memorize and exactly apply the ascent plan with the various decompression stops.
However, given that this device was then adopted on all US Navy submarines for more than thirty years, it is logical to think that the real limits of use of the Momsen Lung were soon understood and regulated by operating procedures more suited to its real performances. We can argue that the actual use of the device no longer included ascents with decompression, but rather a much faster ascent phase and from more modest depths. In the following years the standard depth for exercises would in fact be increased to 50 feet (15 meters). The device that went into production and was adopted by the US Navy is shown in fig. 8 in the hands of Momsen himself.
 |
 |
| fig. 7 | fig. 8 |
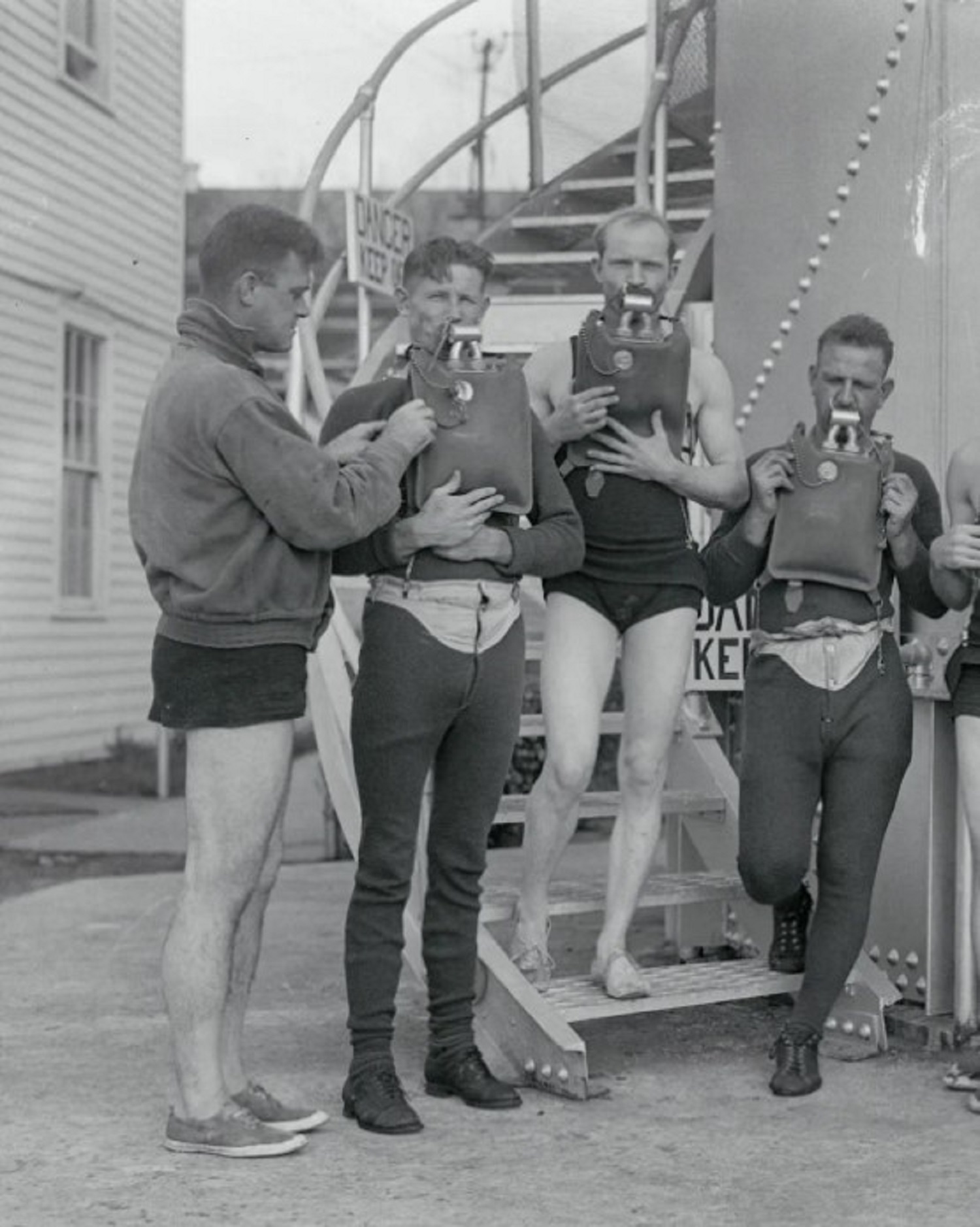
Early from the year the patent application was submitted (1929), the first tests with the Momsen Lung began on US Navy submarines. The fig. 9 shows the group of 26 sailors who successfully carried out an exit and ascent test from an old submarine sunk for this purpose. The photo in fig. 10 was taken in 1930 and is referred to this initial period of testing and training of the crews. Shown here is a crew member equipped with a Momsen Lung, exiting the hatch of the submarine USS V-5 (SC 1).
 |
 |
| fig. 9 | fig. 10 |
In the following years the device was subjected to various modifications and improvements, as shown by the photos in figs. 11 and 12.
 |
 |
| fig. 11 | fig. 12 |
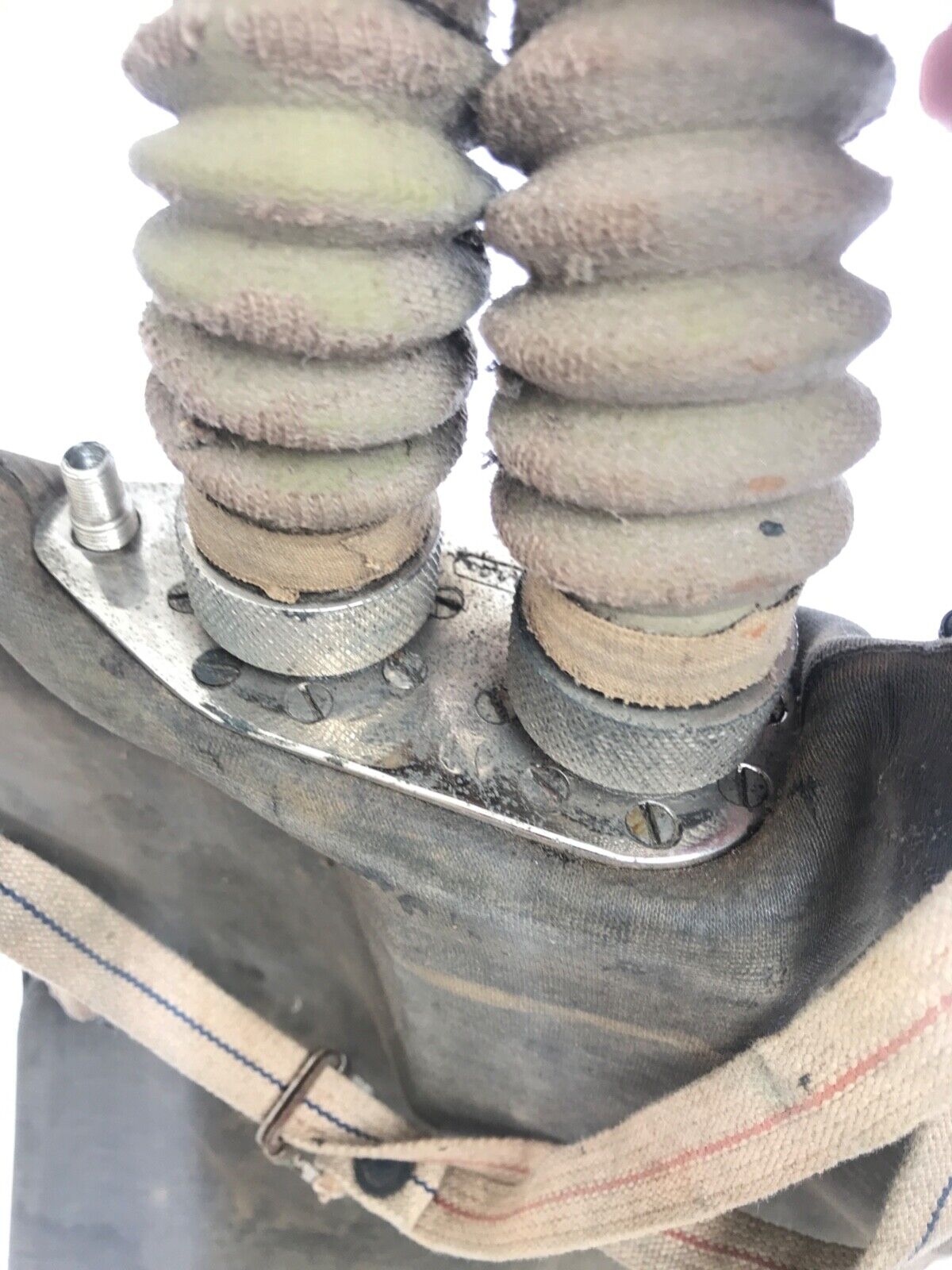
The main modification concerned the position of the lung bag which was progressively raised from the ventral area towards the head of the operator. This decision was certainly motivated by the need to reduce the gas exhaling effort, probably considered excessive. Consequently, the length of the corrugated hoses was also reduced, as can be seen in fig. 11. Next, as shown in fig. 12, the corrugated hoses were even eliminated and replaced by two short shaped metal tubes placed between the mouthpiece and the upper plate connecting the lung bag. The other minor change introduced was the move of the filling valve of the lung bag from its original position to the upper connection plate.
And it is precisely to this phase of upgrade of the device, from the initial version to its definitive configuration, that one of the specimens, that I was able to recently acquire to enrich my historical diving gear collection, belongs.
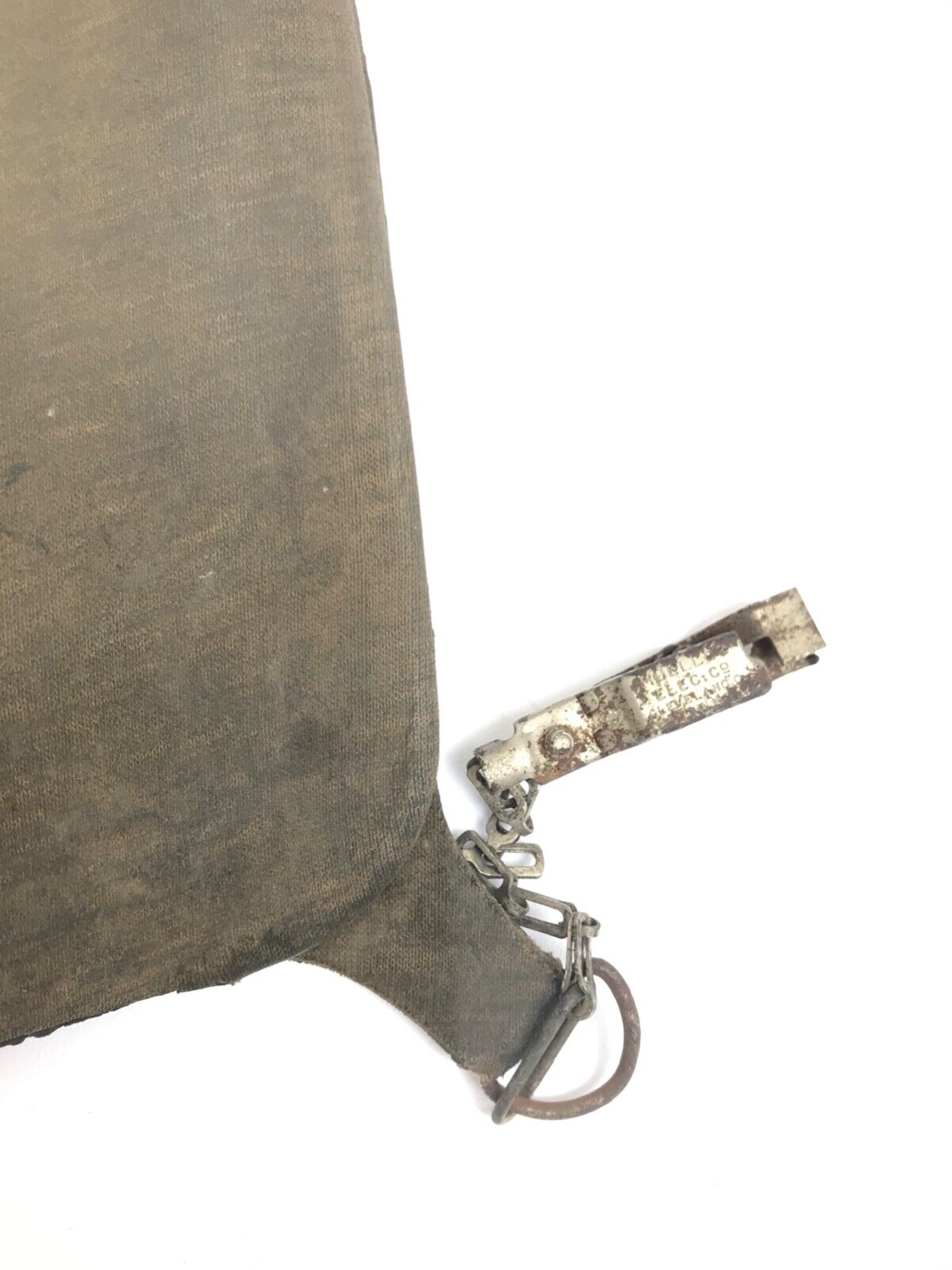
The unit was built by MSA, Mine Safety Appliances and Co. of Pittsburgh Pennsylvania, a company founded in 1914 and specialized in the production of life-saving equipment for several civil and military applications. This particular sample is shown in figs. 13, 14, 15, 16, 17, 18, 19, 20, 21 and 22 and was supplied to the Argentine national navy. As can be seen from the photos, it is in fair condition with the exception of the mouthpiece, which is completely collapsed and reduced to a shapeless body.
 |
 |
| fig. 13 | fig. 14 |
 |
 |
| fig. 15 | fig. 16 |
 |
 |
| fig. 17 | fig. 18 |
 |
 |
| fig. 19 | fig. 20 |
 |
 |
| fig. 21 | fig. 22 |
This version was not the last one, as the real use of the device suggested other updates that had the aim of making the Momsen Lung increasingly more effective, practical and also cheaper. The lung bag was further moved upwards and its shape optimized so as to further reduce the exhaling effort. For the first time in history, the horseshoe shape was proposed in the upper area of the bag, a shape that would later also be used in the famous ARO model 57/B produced by the Italian company Cressi Sub starting from 1957. And finally Momsen understood that for a device like this used for such a short period of time during the ascent phase, the adoption of a cyclic breathing circuit did not bring decisive advantages, in the face of greater construction complexity and higher costs. It was therefore decided to transform the breathing circuit from cyclic to pendulum. The definitive version of the device was introduced into US Navy submarines before the start of the Second World War, as shown in the figs. 23 and 24.
 |
 |
| fig. 23 | fig. 24 |
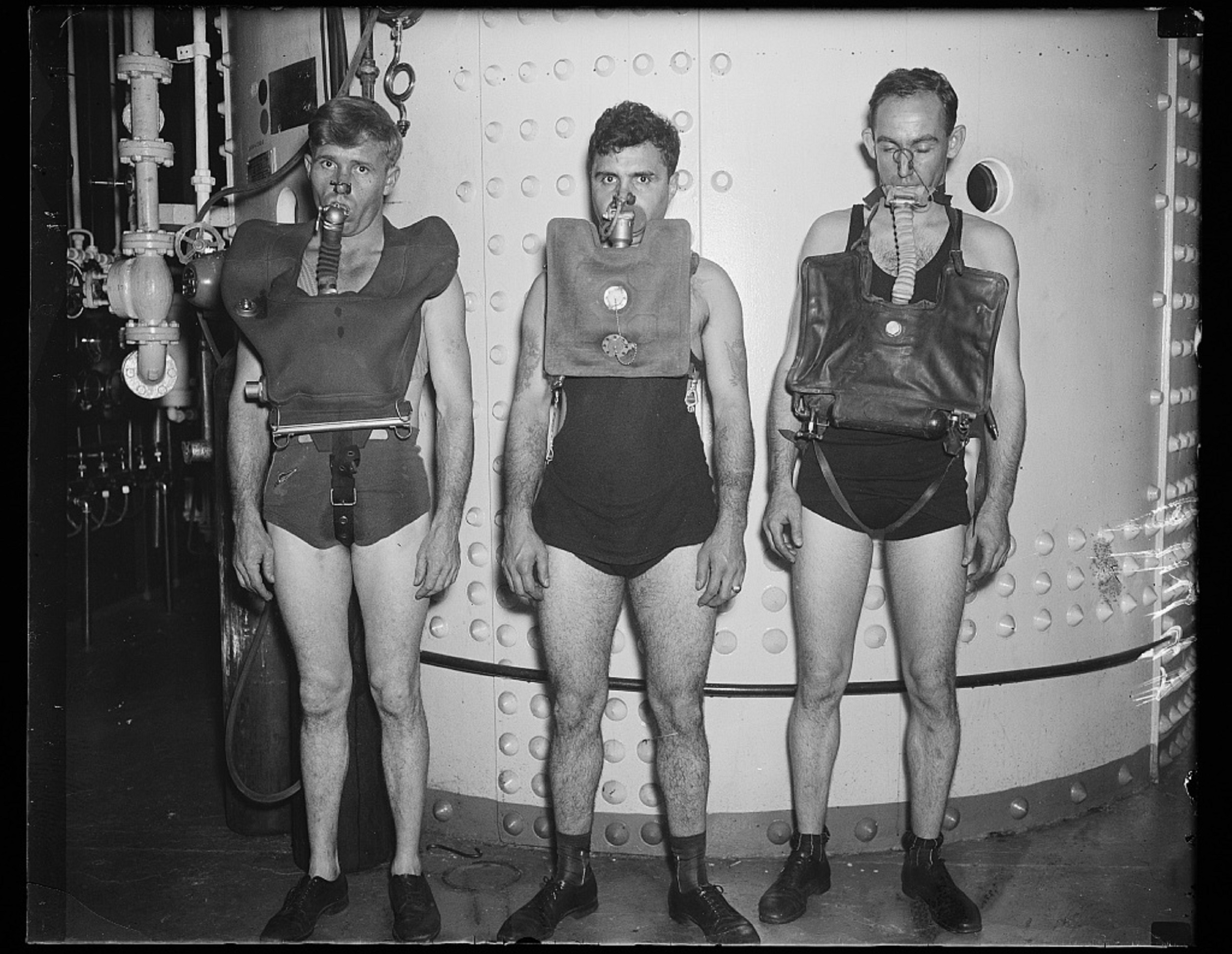
The detail of the new mouthpiece and the new hose of the pendulum breathing circuit is shown in fig. 25. The Momsen Lung, in its final version, is shown in the center of the fig. 26 together with its competitors used by the main navies of Western countries during the Second World War, the German Gegenlungen (Tauchretter), produced by Dräger (on the left), and the British DSEA produced by Siebe & Gorman Ltd (on the right).
 |
 |
| fig. 25 | fig. 26 |
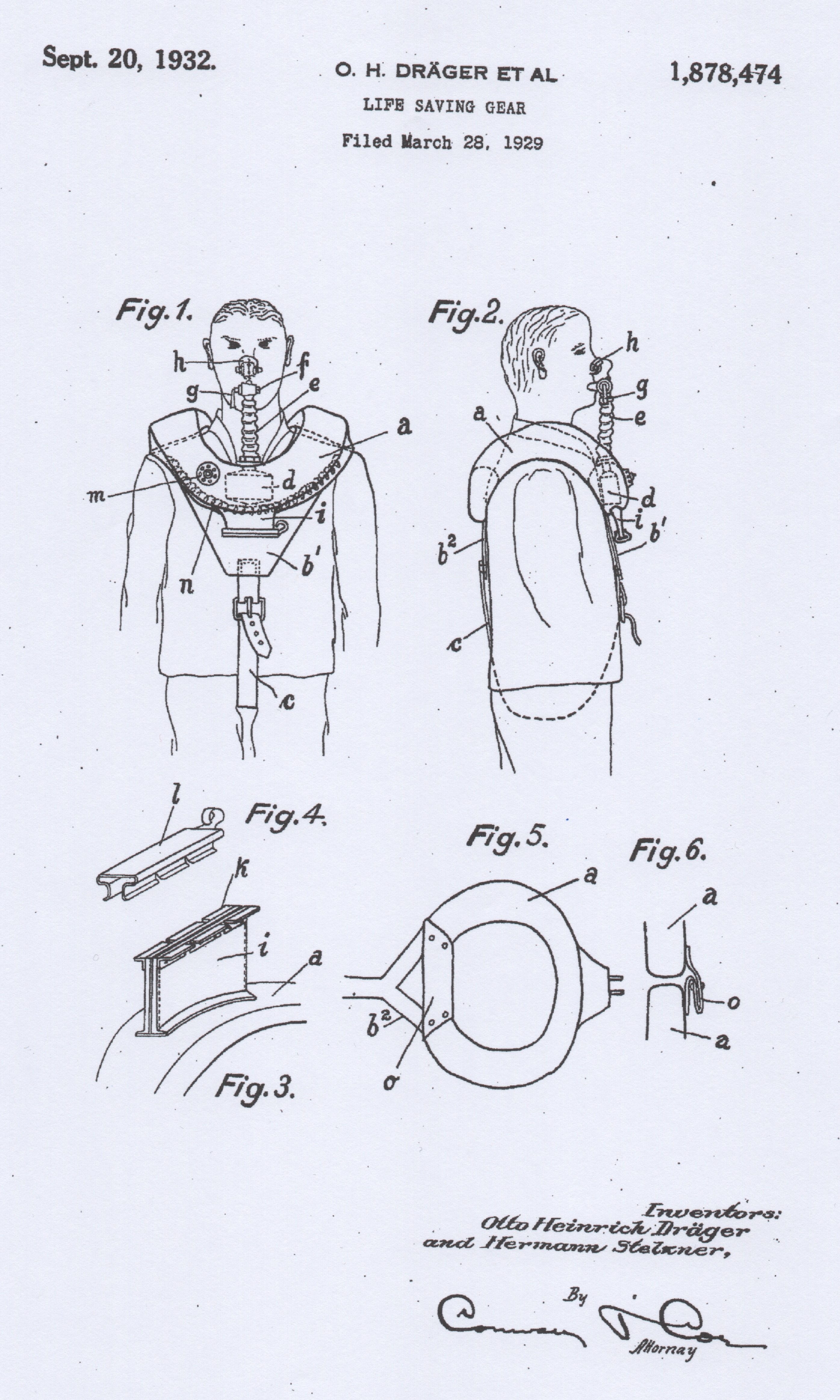
Upon closer inspection, even the configuration of the German devices used during the war was not very different from that of the US breathing unit. In fact, this device was patented in the USA almost at the same time as the Momsen Lung, as we can see in fig. 27. Apart from the configuration of the lung bag and harness, the only substantial difference with the US apparatus was the content of the canister. In fact in its prototype version, instead of being provided with simple soda lime, it was filled with sodium peroxide, a chemical substance which, in addition to fixing carbon dioxide, is capable of producing oxygen. Thanks to this characteristic, the Tauchretter (see the unit in fig. 28 recovered from the German submarine U-877) was able to ensure greater availability of oxygen during the ascent to the surface, however with a greater inherent risk in the use of sodium peroxide (an extremely caustic substance capable of producing serious burns in case of contact with parts of the body and the human respiratory system).This solution, which would later be widely adopted by the Soviets in the construction of numerous models of rebreathers for similar uses, was soon scrapped and replaced with the classic tank filled with oxygen and a canister containing simple soda lime.
 |
 |
| fig. 27 | fig. 28 |
The second sample of Momsen Lung recently entered my collection and shown in figs. 29 - 30, is part of the last production batches of this device.
 |
 |
| fig. 29 | fig. 30 |
The only true and documented experience of use of this device with partially positive results is that of the rescue of the crew members of the US Navy submarine USS Tang which sank on 25 October 1944. Of the 13 crew members (out of a total of 30) who attempted to ascend with the Momsen Lung, only 5 were capable to reach the surface safely, but they were then captured and imprisoned by the Japanese. This episode is mentioned in Clay Blair Jr.'s book “Silent Victory: The U.S. Submarine War Against Japan – January 30, 2001”.
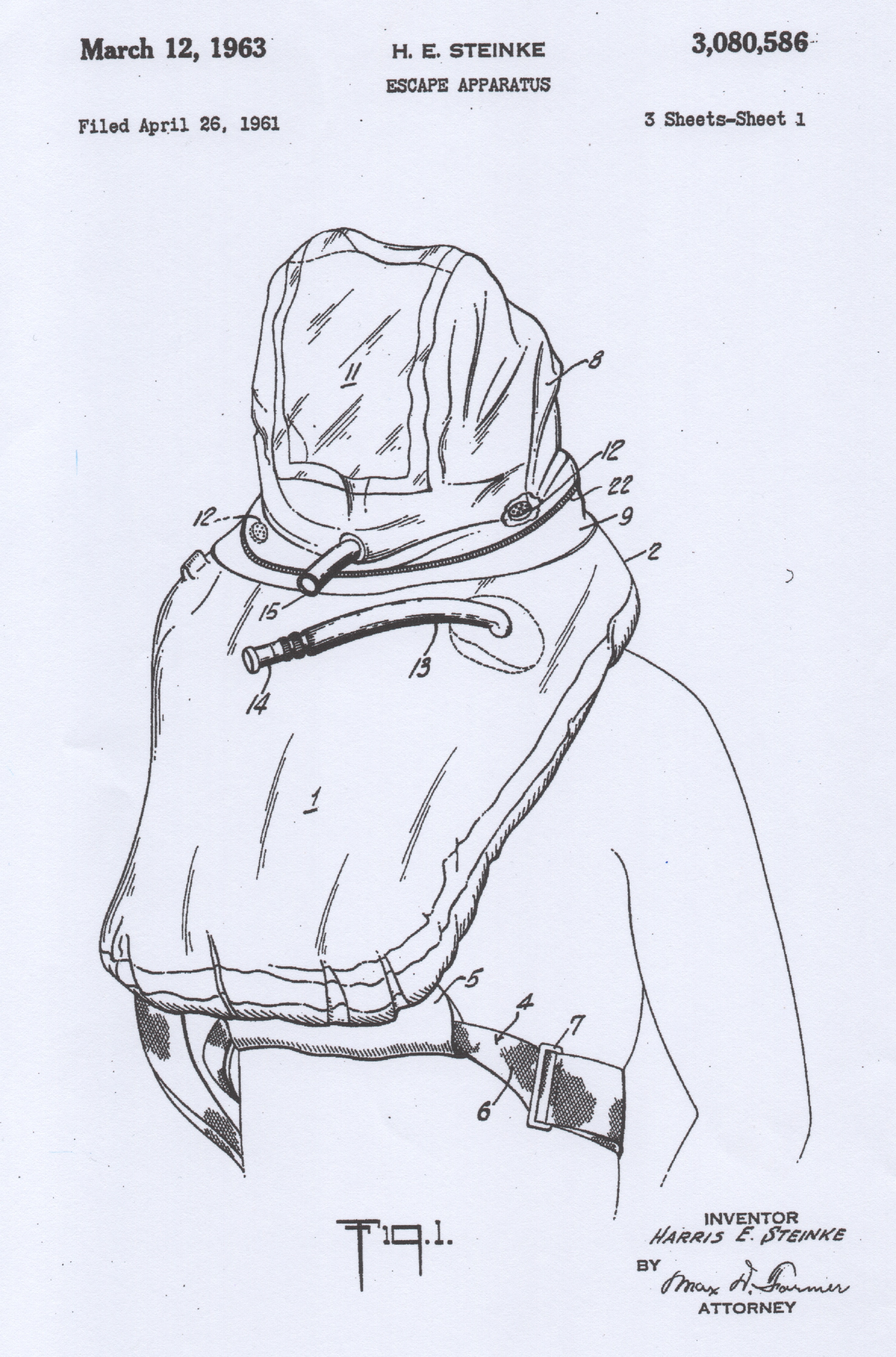
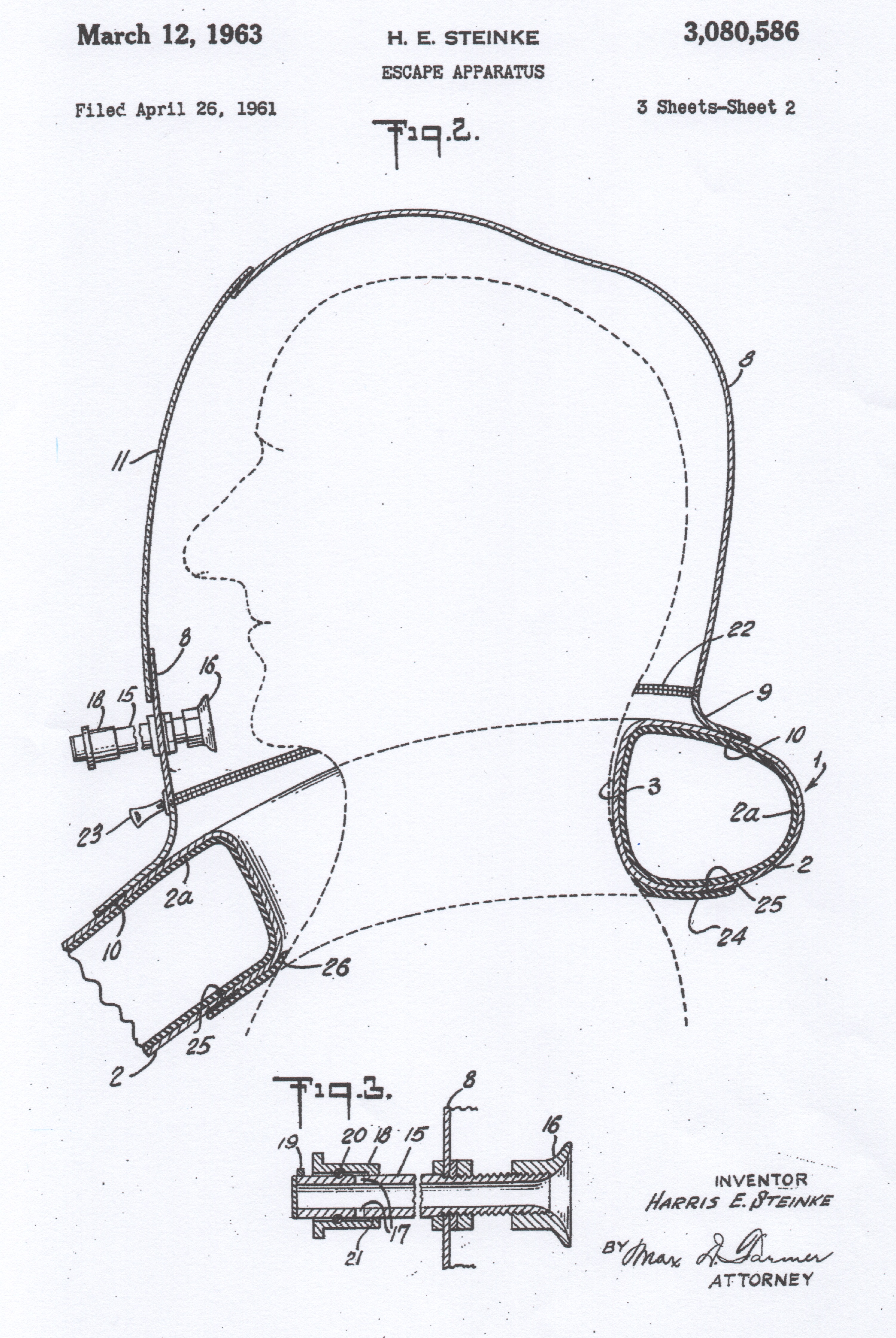
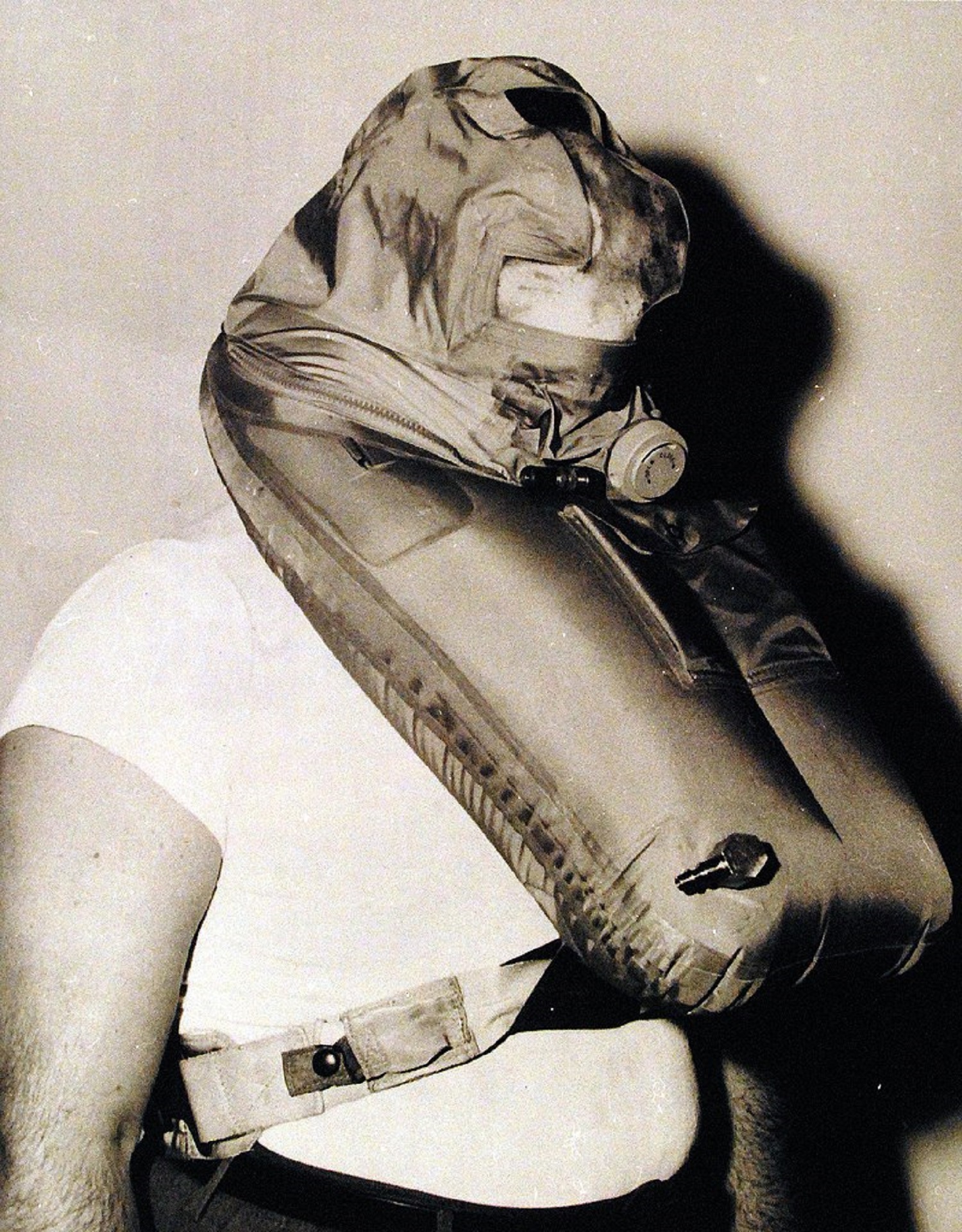
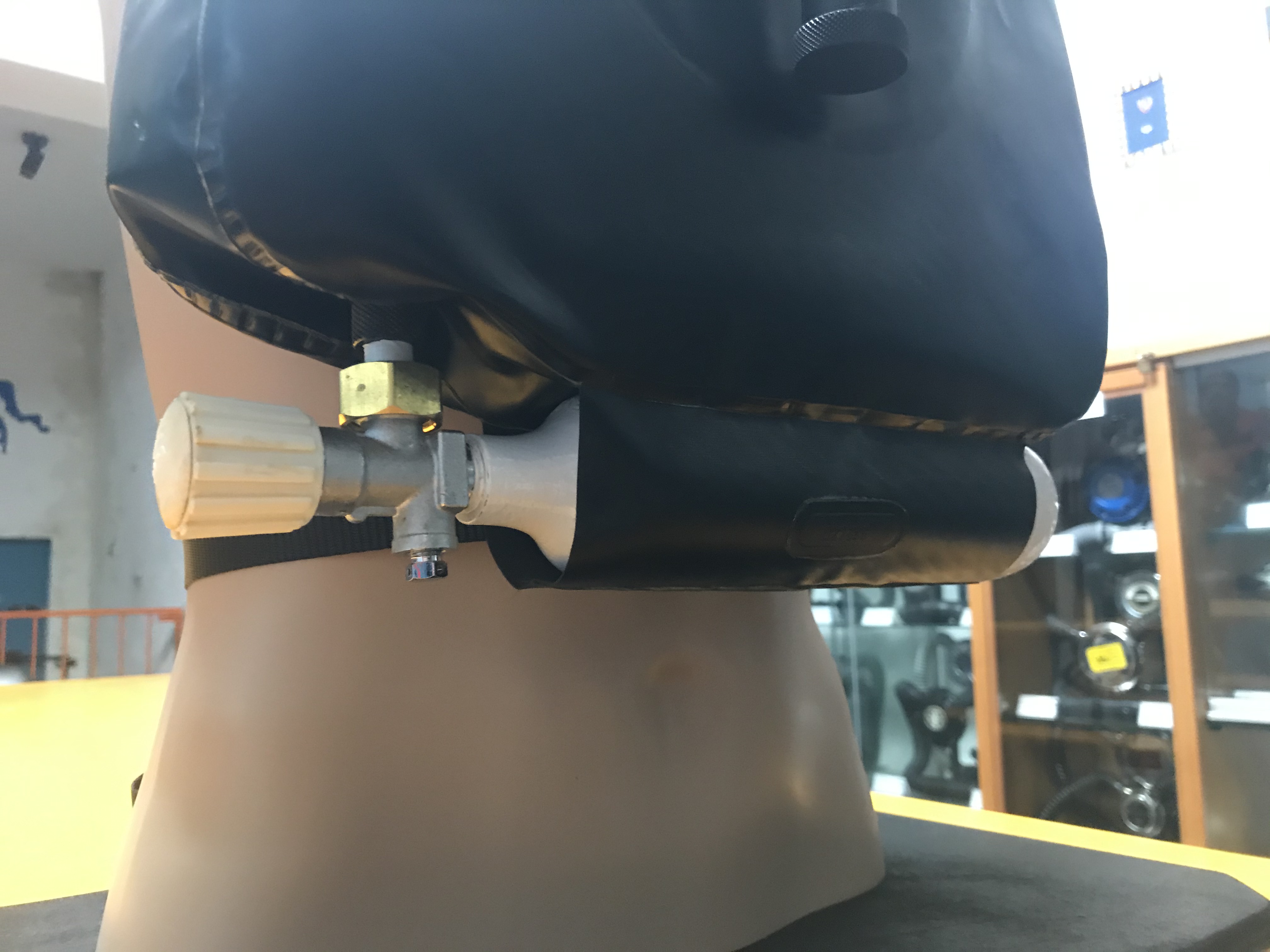
The Momsen Lung remained in use with the US Navy until the early 1960s when it was replaced with the Steinke Hood, patented in 1963 by the US Navy Lieutenant Harris E. Steinke (fig. 31 - 32- 33 - 34).
 |
 |
| fig. 31 | fig. 32 |
 |
 |
| fig. 33 | fig. 34 |
This device worked in a similar way of the Momsen Lung, in the sense that it did not include tanks for the supply of breathing gas during the ascent phase, but compared to the previous device it did not have any canister for soda lime, with all the advantages in terms of costs and reduction of periodic maintenance. The air for the operator's breathing was produced by the expansion of the gas contained in the lung bag and then discharged through small maximum pressure valves inside the watertight hood, equipped with a transparent window and a snorkel for breathing inside the submarine and after reaching the surface. The other advantage of the Steinke Hood was that the operator could breathe naturally through the nose with less risk of lung overdistension.
After the war there were other lines of development of these devices which followed the construction and functional scheme of the DSEA, but which could use the new materials and technologies available and the more advanced knowledge of physics and physiology in a hyperbaric environment.
The unit shown in fig. 35, 36, 37 and 38 was produced in the UK during the 1980s (unfortunately I was unable to identify the manufacturing company). As can be seen, the operating principle has remained similar to that of the DSEA (lung bag with soda lime canister inside, pendulum type breathing circuit, mouthpiece with neck strap, glasses and nose clip), but with some substantial changes compared to that. The tank (fig. 36) no longer contained oxygen but compressed air (or Nitrox) to allow a higher operational depth, so reducing the risks associated with breathing hyperoxic gas mixtures, and delivered a constant flow of gas in order to replenish the quantity of oxygen consumed by the operator's metabolism. The excess gas delivered by the tank or simply produced by the volumetric expansion in the lung bag during the ascent, was discharged through the maximum pressure valve shown in the fig. 38.
 |
 |
| fig. 35 | fig. 36 |
 |
 |
| fig. 37 | fig. 38 |
The Steinke Hood remained in use by the US Navy until the end of the first decade of the 2000s. Although it proved to be an excellent performing device, its limitation was that it did not provide any type of thermal protection to the operators both during ascent and during floating phase on the surface when waiting for rescue units. This limit could prove fatal for personnel in cold water conditions even with exposure times of just a few minutes. Solutions were therefore developed that made it possible to improve both the thermal protection aspect and that of surface flotation. Various configurations of the new device were developed which was called SEIE (Submarine Escape Immersion Equipment) and adopted by the US Navy and many other navies of Western countries (it is also in use today). This device, of which we see some photos in fig. 39 and in fig. 40, is approved for evacuations from submarines up to a depth of 600 feet (183 meters) with an ascent speed of 2-3 meters per second and the possibility of evacuating more than eight crew members every hour (this last number is limited by operational capabilities of the submarine's escape lock). As we can see, the equipment includes a full wetsuit for the protection of the entire body and, in some versions, also an inflatable boat in order to improve the flotation and comfort of the operator while waiting for rescue units.
 |
 |
| fig. 39 | fig. 40 |
The lines of development of the equipment that we have described in this article and which have seen the Momsen Lung among the main protagonists of the devices intended for the recovery of the crews of sunken submarines, are significantly different from those undertaken by the navies of the former Soviet bloc after the end of the Second World War. The objective of creating equipment with a good compromise between effectiveness, ease of use and reasonable costs was evidently not considered fundamental for the Soviets who, on the contrary, created very complex and very sophisticated equipment with extreme declared performances absolutely incredible in terms of operational depth. The solutions they proposed were several and some were truly complex and potentially dangerous (e.g. semi-closed SCR rebreathers with automatic mechanical systems for regulating gas flows and oxygen-generating filters operating on peroxide, etc.). But this is another story that perhaps we will tell in a future article.